

Abstract
The six-minute walk test (6MWT) was introduced in adults and children suffering from pulmonary or cardio-vascular conditions to assess their sub-maximal functional exercise capacity. In sickle cell disease (SCD), a reduced 6-minute walk distance was observed in adults with chronic pain, hip avascular necrosis and osteopenia ; and in children with low hemoglobin level, low fetal hemoglobin, a baseline elevated TRV. In a previous study (Dedeken et al., PLoS One 2014), we also showed that abnormal 6MWT was significantly associated with the presence of silent infarct.
The aim of our study is to explore the evaluation of the 6MWT over time and to confirm the correlation with the cerebral vasculopathy in a larger cohort.
This study was conducted at Hôpital Universitaire des Enfants Reine Fabiola (Brussels, Belgium) and included SCD children older than 6 years, regularly followed between 2011 and 2017 and who had at least two 6MWT. The age-standardized predicted value of the 6-minute walk distance (6MWD) was established as reported by Geiger. The 6MWT was considered as normal if the 6MWD was more than 80% of the age-standardized predicted value. Baseline hematological values, clinical events, cerebro-vascular disease, cardio-pulmonary parameters and disease-modifying treatment (DMT) were compared between those with normal and abnormal 6MWT and according to the 6MWD and between the 1st and the 2nd 6MWT overtime.
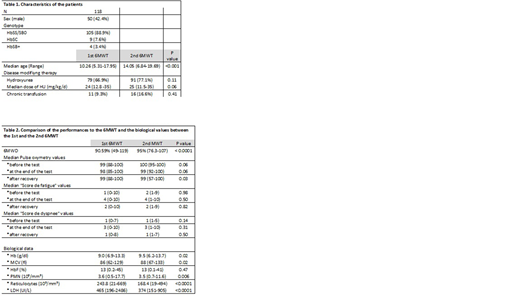
118 patients have been assessed twice and had at first evaluation a 6MWD of 90.6% (Range 49-119%), with an abnormal test found in 5.1%. The characteristics of the patients are detailed in the Table 1. The changes of the 6MWD and the biological data over time are detailed in Table 2. After 4 years of follow-up, 77.1% of patients were treated with Hydroxyurea (HU) and 16.6% patients were chronically transfused. In parallel with the increased HU prescribing rate, we have observed a significant increase of the Hb and the MCV and a decrease of reticulocytes and hemolysis parameters. The first 6WMT was performed at the median age of 10.3 years and the last one at the median age of 14.1 years. The median 6MWD increased over time including for non-chronically transfused patients. Girls performed less well in the 6MWT (93% for girls vs. 95.7% for boys; P = 0.03). Acute chest syndrome was significantly more frequent in boys (62%) compare to girls (38.7%). Nevertheless, no other differences were founded between boys and girls regarding biological values, clinical events or DMT. 26.5% of our patients have silent infarcts at a median age of 14.6 years. The 6MWD was the same in patients with and without silent infarcts (92.5% vs. 95% ; P=0.17) even when chronically transfused patients were excluded (94% vs. 95% ; P= 0.20). Patients with silent infarcts have a significant lower hemoglobin level and higher reticulocytes count, neutrophils count, LDH and MCV.
In conclusion, the 6MWD observed in our cohort characterized by a very high rate of HU treatment is much higher than published in others series and improved over time. With only 5% of SCD patients having a 6MWD < 80% of the normal predicted value at last evaluation, we were not able anymore to confirm a correlation between the presence of silent infracts and abnormal 6MWT.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal